

Nick TriggleHealth correspondent
 BBC
BBCAs ambulances queued in front of Royal Berkshire Hospital in Reading last week, corridors full of patients were waiting for a bed on a ward. Emergency department consultant Omar Nafousi was at his wit’s end.
“We’ve no space,” he told the BBC last week. “This is not what I signed up for when I became a doctor.”
It is a scene that is being repeated in hospitals up and down the country as winter viruses and cold weather add to the pressures on the health service.
Currently nearly 4,000 beds in England alone are taken up by patients with flu, Covid and the vomiting bug norovirus, according to NHS England, and the situation is on a similar scale in the rest of the UK.
But that is dwarfed by another pressure – the patients who should not be in hospital.
 In Pictures via Getty Images
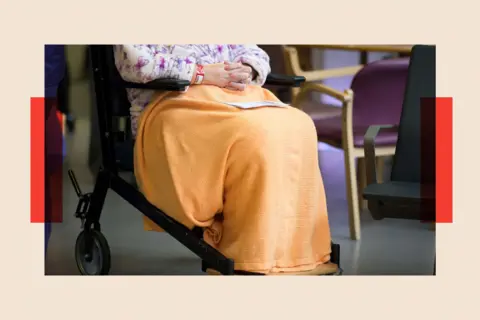
In Pictures via Getty ImagesEvery day there are more than 13,000 people whose treatment has been completed who are still in hospitals in England, the latest figures from NHS England suggest. Plus there are a further 4,000 around the rest of the UK – which means around one in eight beds are occupied by people who don’t necessarily need to be there.
Many of these “delayed discharge” patients are older and may be frail and living with multiple health conditions who need support in the community.
But it comes at a huge cost. The average hospital bed takes £562 a day to staff and maintain, according to NHS England, meaning the health service in England is losing more than £225m a month supporting patients who could be elsewhere.
Then there is the cost to other patients.
“We are seeing surgery cancelled and long waits in A&E because there are no beds available on the wards,” says Clifford Kilgore, a senior nurse working with older people, who serves on the Nurses and Allied Health Professionals’ Council of the British Geriatrics Society.
As for the staff there is a toll on morale, too – among doctors, nurses and ambulance workers. “It’s terrible when you see patients go downhill in hospital when you know they would be better off somewhere else,” says Laura Hichens, a nurse who leads the “discharge liaison” team at Queen Elizabeth Hospital in Gateshead.
The issue of delayed discharges is far from new. For years, it has been talked about, if not agonised over, and the NHS started tracking the delays in the early 2010s. Last summer, the government launched an urgent and emergency care plan, which pledged to reduce the delays, with the promise there would be improvements.
If it could be solved, the impact on the NHS would be transformative, experts have told me.
Yet the problem throws up many deeper questions about the care system, coordination and planning in hospitals – with some doctors even asking whether the NHS is over-treating patients, particularly those at the end of life.
‘The system’s running faster just to stand still’
On paper, it all sounds straightforward: simply send all those patients who are well home. But it’s not that easy.
“It takes a lot of time and effort to discharge a patient,” says Emma Dodsworth, a researcher who has studied the issue for Nuffield Trust think tank. “Some may need adaptations to their home, some short-term help with washing and dressing or home visits from nurses. Some a combination of all three, while others may need a care home place to be found.
“And because the population is getting older and frailer, there are more complex cases ending up in hospital. The system is having to run faster just to stand still.”
Arranging the discharge of these patients relies on a close relationship between council-run social care services and the NHS.
 Getty Images
Getty ImagesThere are plenty of examples of this happening. At Gateshead’s Queen Elizabeth Hospital social workers and nurses are working side-by-side in the discharge liaison hub, which has been fully up and running for two years. The hub also has a housing officer, employed by the council, to arrange home adaptations or temporary housing.
Planning for discharge begins as soon as a patient is admitted to hospital. “That means when they are ready to be discharged it can be done pretty much straight away for many,” says Hichens.
Figures show the hub consistently discharges patients more quickly than average.
It’s a template that some might suggest should be rolled out en masse across the country – but so far that hasn’t happened.
‘Strained relations’ with social care
A recent report by the NHS Confederation and Association of Directors of Social Services (ADASS) warns that cooperation between the NHS and social care sectors is “inconsistent” across the country with relationships sometimes becoming “frictional”.
Kerrie Allward, who acts as a policy lead for ADASS and is executive director for adult social care and health at Walsall Council, is not surprised by these findings.
Her area has adopted a similar approach to Gateshead and she says that led to a five-fold drop in delayed discharges in the year after it was introduced.
But she argues that across the social care sector money remains a “critical issue” – with local government funding squeezed so much over the past decade or so that spending on social care has not been able to keep up.
Local authorities are spending around £32bn a year on adult social care – that is £4.6bn higher in real terms than 2010-11 – but councils argue that increase has been swallowed up by higher costs, increasing demand and greater complexity of need.
 NurPhoto via Getty Images
NurPhoto via Getty ImagesAllward says some councils have tried to compensate by spending ever more on social care – which now accounts for more than half of their budgets across the board. But, she says, “Councils often lack the funds to invest in integrated services that would support more timely discharge.”
And while she enjoys working with the NHS, in her experience not all social care directors feel the same – she says that some NHS leaders blame social care for delayed discharges.
“This blame can strain relationships, especially as data reveals that social care is usually responsible for only a minority of delays.”
The government said it was increasing investment further in the coming years, while seeking wider reform of the way services are funded.
Examining the Danish approach
Some other European countries have a different approach.
Denmark, for example, has created a national network of “intermediate care beds” in community hospitals and care homes, staffed by nurses and carers, that patients can be discharged into.
Denmark has also invested in community nursing services to support patients in the community and in their homes rather than in hospital.
“We could learn from places like Denmark where there is much greater integration between health and social care,” says Dodsworth.
 Getty Images
Getty ImagesSome NHS trusts have bought places in care homes to allow them to discharge patients. University Leicester Hospitals NHS Trust has taken this one step further: it has spent £10m buying and renovating a former care home in the city called Preston Lodge, which opened in July and has more than 50 beds.
Staffed by nurses, physiotherapists, occupational therapists and with its own GP, it allows patients who are medically fit to leave hospital continue to receive support. Preston Lodge says these patients would have spent an extra 10 days in hospital on average.
Inside Preston Lodge, patients eat meals together and some of them socialise, too – doing jigsaw puzzles and watching TV together.
“Hospitals are great places when you are acutely ill, but they are not when you no longer need that medical care,” says the trust’s head of nursing Emma Roberts.
Dodsworth says these “step-down” facilities can help patients get back on to their feet while not taking up a hospital bed.
However, she says the lack of integration between social care and the NHS remains an obstacle to this approach being used more widely.
The question of family responsibility
Improving coordination between the NHS and councils is only part of the solution, however. NHS England monthly data shows that around only a third of delays are down to lack of community care or a care home place.
Another challenge is the attitude of some families who prefer – and feel safer, perhaps – if their loved one is under the care of a hospital.
Hichens says she spends much of her time persuading the family members of patients that they would be happier elsewhere – and healthier too.
“They think hospital is the best place for their relative,” she says. “But we know the longer you spend in hospital the more patients are at risk of getting frailer, losing strength and needing more care.”
Some families are not prepared to take on caring responsibilities either, says Dr Vicky Price, an acute medical consultant who diagnoses and treats patients brought in as emergency admissions.
“In some countries, the culture is different – they don’t need care homes because families step in.”
But she concedes it can be difficult for some families, including financial pressures that make caring for a relative a challenge. “There are justifiable reasons why they can’t take on that responsibility.”
Time to rethink end-of-life care?
In Price’s view, her own profession bears some responsibility, too. She says about a third of people who are admitted for medical reasons are in their last year of life.
“We admit them and end up over-treating them with interventions, scans and pills,” argues Price, who is president of the Society for Acute Medicine.
One patient she saw recently was in his late 80s and had 14 appointments booked for the next two months for health problems including cardiac and renal issues, and liver and eye problems.
“I talked to him – the only one he really wanted to keep was the eye one,” she says. “We cancelled the rest.
“The problem when you start trying to treat everything is that you prescribe more pills, those pills have side-effects and you can actually end up making a person’s health worse.”
 Heritage Images via Getty Images
Heritage Images via Getty ImagesDoctors often lack the confidence as well as the time to have these difficult discussions with families, Price says.
But changing that approach would also raise numerous ethical questions.
She says for many of these patients, palliative care and managing their symptoms, mainly pain, would be preferable: “Their quality of life would be much better and we would avoid a hospital admission.”
But in practice there are obstacles to this.
And the Association of Palliative Medicine has long argued there is insufficient investment in end-of-life care, which means people struggle to get support. Marie Curie suggest nearly a quarter of people who need palliative care do not get it.
Clifford Kilgore agrees reducing admissions is a key part of the solution. “Hospitals are good for treating an acute illness, but the problem is that if you admit an older person with pneumonia they can spend a week in a hospital bed not moving and they become immobile and unable to look after themselves,” he says.
“It is a vicious cycle. For some patients, being in hospital actually causes harm.”
He helps to run a “hospital-at-home” service, which provides specialist hospital-level care to patients with frailty and conditions such as heart failure and respiratory illness.
Services of this kind care for around 12,000 people around the country, but again they are not available everywhere. Providing more expert care like this outside of hospital is a priority for the NHS under the government’s 10-year plan.
Kilgore says it cannot come soon enough: “Get this right and it would have an immediate impact.” But not soon enough for those patients in Reading queuing for a bed.
Top picture credit: LightRocket via Getty Images

BBC InDepth is the home on the website and app for the best analysis, with fresh perspectives that challenge assumptions and deep reporting on the biggest issues of the day. You can now sign up for notifications that will alert you whenever an InDepth story is published – click here to find out how.
Source link : https://www.bbc.com/news/articles/c394vjm7n4vo?at_medium=RSS&at_campaign=rss
Author :
Publish date : 2026-01-12 00:08:00
Copyright for syndicated content belongs to the linked Source.













{kind=link}