
Dr. Tanzira Zaman and Dr. Ekaterini Zapantis partnered with Boehringer Ingelheim to share the health messages below. Dr. Zaman and Dr. Zapantis are paid consultants for Boehringer Ingelheim.
Idiopathic pulmonary fibrosis (IPF) and progressive pulmonary fibrosis (PPF) are progressive conditions that can cause continuous decline in lung function.1,2 While IPF’s root cause is unknown, PPF is linked to an underlying clinical interstitial lung disease (ILD) diagnosis — like autoimmune disorders or environmental exposures or can also arise from unknown causes.1,2,3
Affecting hundreds of thousands in the U.S., patients may dismiss the symptoms of pulmonary fibrosis or mistakenly attribute them to factors like fitness level or aging.4,5,6,7 Nonspecific symptoms also lead to misdiagnosis.7
“Diagnostic delay and misdiagnosis remain common with IPF and PPF. These represent conditions in which we have already seen and/or expect clinical worsening,” says Tanzira Zaman, MD, Medical Director, Interstitial Lung Disease Program, Cedars-Sinai. “That’s why it’s important to diagnose these conditions sooner.”
“Delays in diagnosis allow further loss of lung function,” says Ekaterini Zapantis, MD, Managing Partner and Chief Medical Officer, Rheumatology Center of WNY. “Management of my patients with PPF is highly collaborative, utilizing shared decision-making with pulmonologists.”
Exploring IPF and PPF Care
Treatment options for IPF or PPF have historically been limited, until late 2025 when the U.S. Food and Drug Administration (FDA) issued approvals for JASCAYD® (nerandomilast) tablets for the treatment of adults with IPF and also for adults with PPF.8,9
IMPORTANT SAFETY INFORMATION
ADVERSE REACTIONS
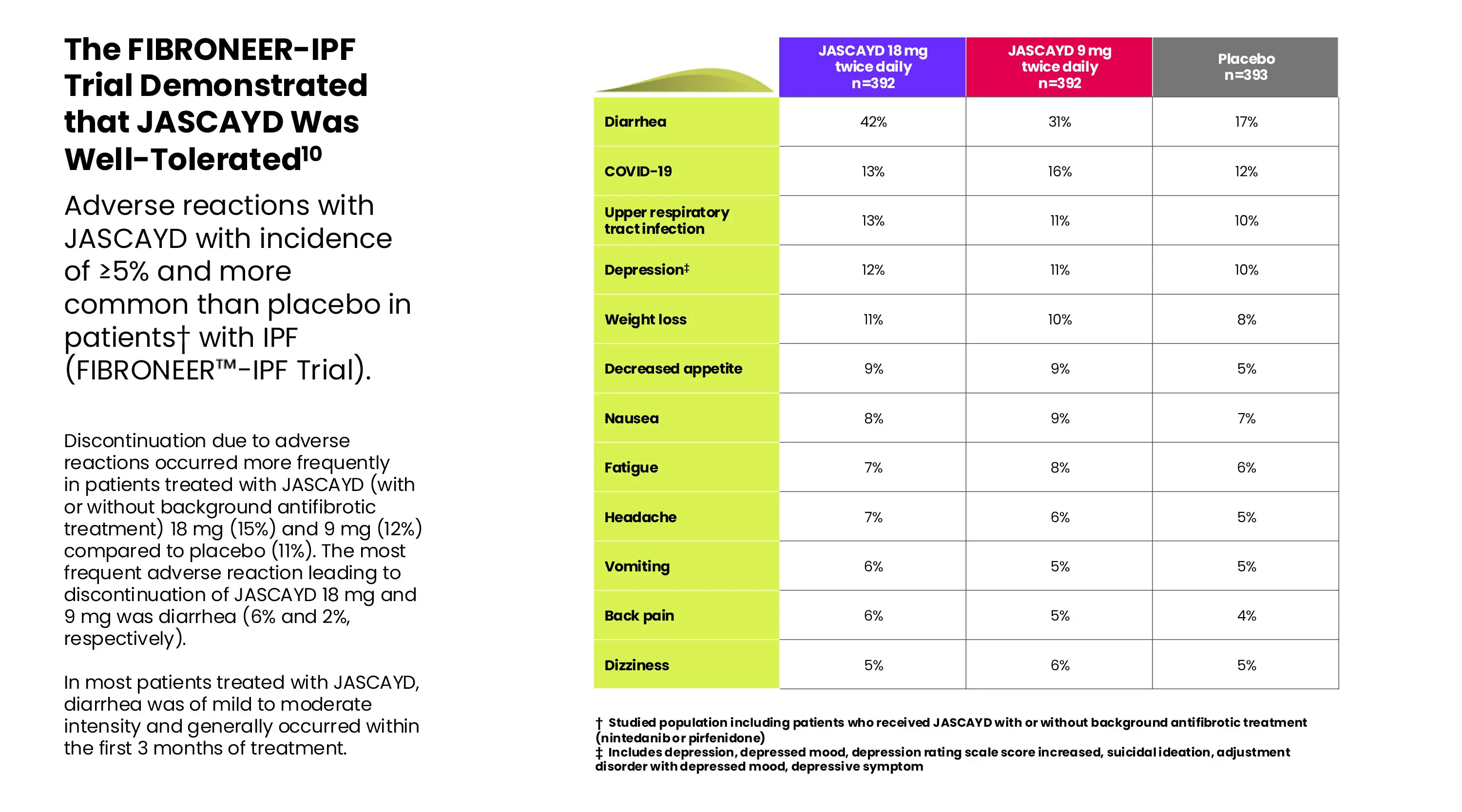
- The most common adverse reactions with an incidence of ≥5% in patients treated with JASCAYD were diarrhea, COVID-19, upper respiratory tract infection, depression, weight decreased, decreased appetite, nausea, fatigue, headache, vomiting, back pain, and dizziness.
Please see additional Important Safety Information below.
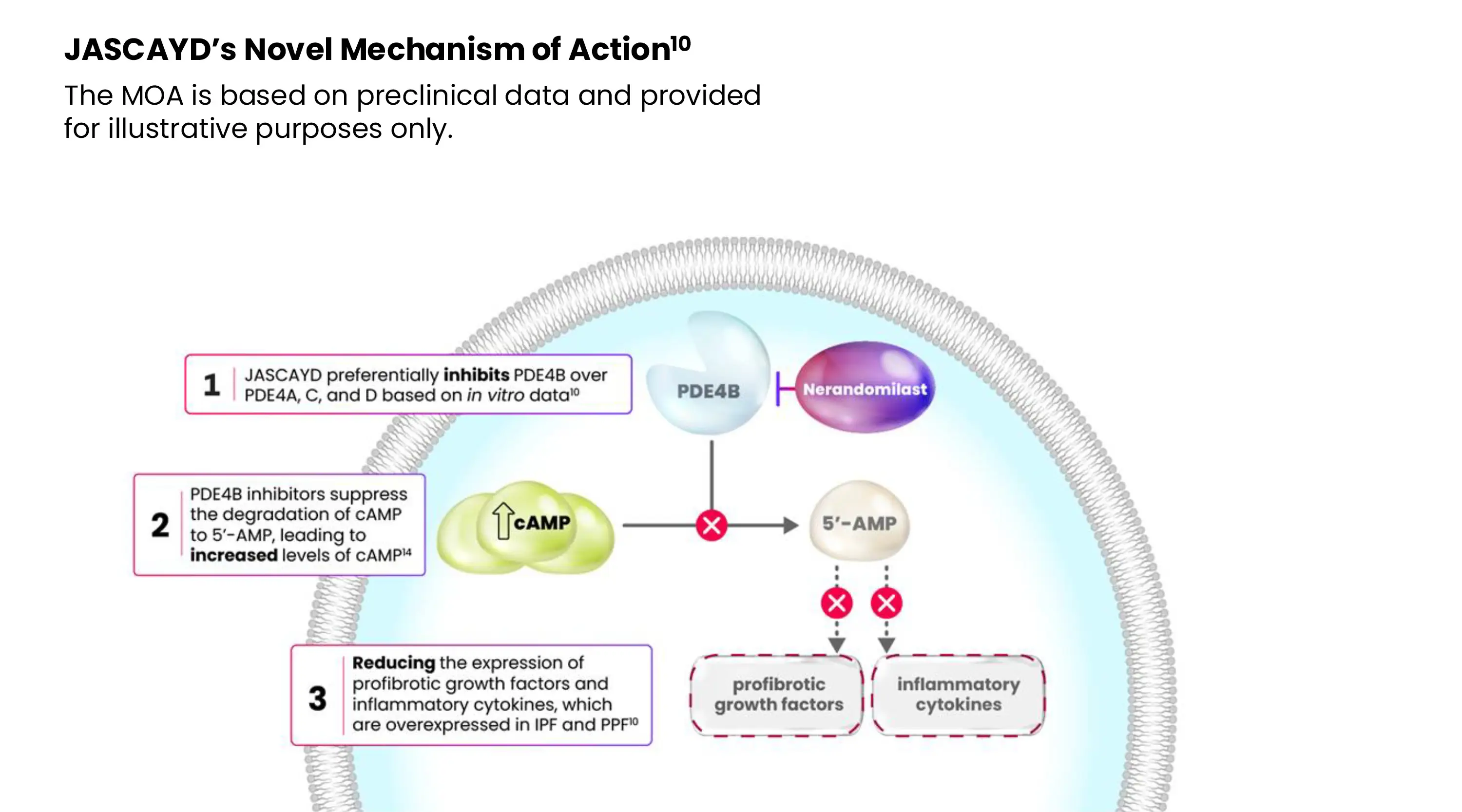
JASCAYD is the first and only preferential inhibitor of phosphodiesterase 4B (PDE4B) approved by the FDA for adults with IPF or PPF.10,11,12,13 JASCAYD inhibits phosphodiesterase 4 (PDE4) with at least nine-fold preferential inhibition of the PDE4B isoenzyme. JASCAYD exerts both anti-fibrotic and immunomodulatory effects, thereby slowing the decline in lung function in IPF and PPF patients.10
Pivotal Data Supporting JASCAYD in IPF
The FDA approval of JASCAYD in IPF was based on data from FIBRONEER™-IPF and Trial 2.10
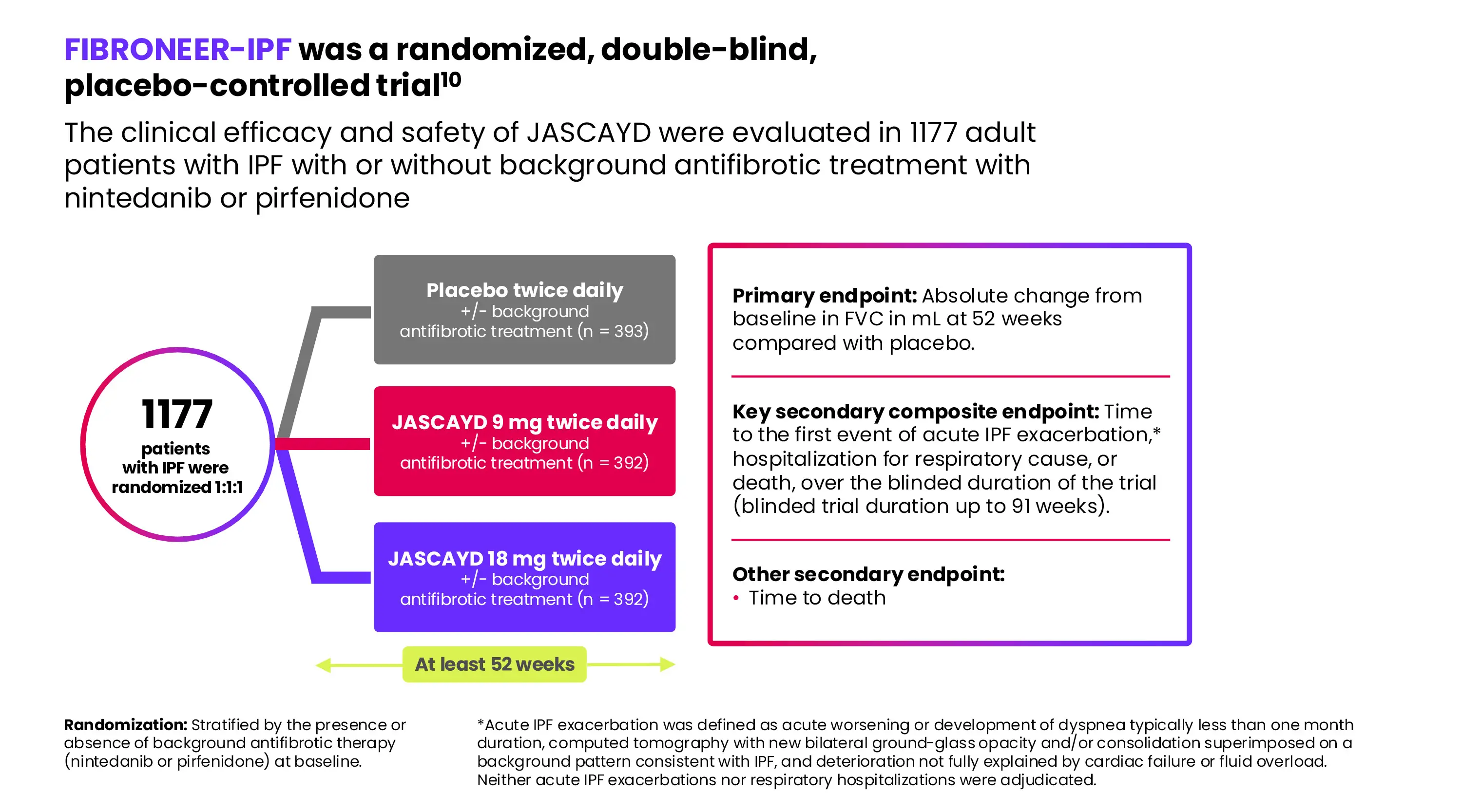
At 52 weeks, JASCAYD showed significantly less FVC decline versus placebo in adults with IPF.10 Patients receiving JASCAYD 18 mg or 9 mg showed average FVC reductions of 106 mL and 122 mL, respectively, versus 170 mL with placebo. The respective treatment differences compared with the placebo group were 64 mL (95% CI: 25, 102) and 48 mL (95% CI: 10, 86).10
No statistically significant difference was observed for the key secondary composite endpoint (JASCAYD 18 mg and 9 mg, respectively: HR 1.17 [95% CI: 0.86, 1.59] and HR 1.03 [95% CI: 0.75, 1.41]).10
In a prespecified exploratory analysis of overall survival, the hazard ratio for all-cause mortality, assessed until the end of trial (up to 109 weeks), did not show a significant treatment difference for JASCAYD 18 mg or 9 mg compared to placebo (HR: 0.66 [95% CI: 0.41, 1.08] and HR 0.95 [95% CI: 0.61, 1.49], respectively).
Trial 2 was a 12-week trial that enrolled a total of 147 adult patients with IPF with or without background antifibrotic treatments (nintedanib or pirfenidone) and were randomized 2:1 to receive JASCAYD 18 mg or placebo twice daily.
In Trial 2, patients taking JASCAYD 18 mg twice daily compared to placebo, with or without background antifibrotic treatments, had a reduction in FVC decline at Week 12 of 91 mL (95% CI: 44, 138).
Pivotal Data Supporting JASCAYD in PPF
The FDA approval of JASCAYD in PPF was based on data from FIBRONEER™-ILD.10
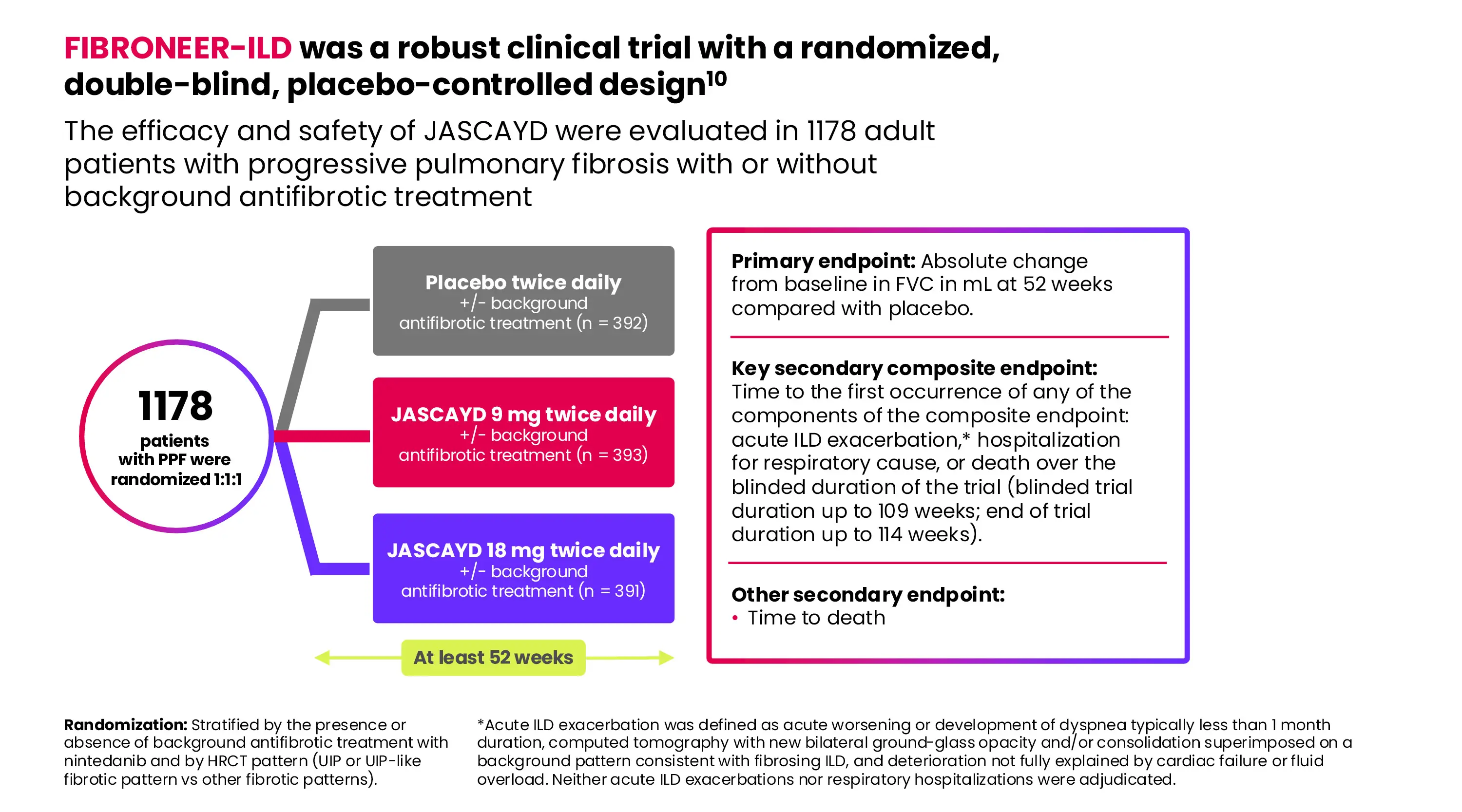
At 52 weeks, JASCAYD demonstrated a significantly smaller decline in absolute change from baseline in FVC compared to placebo in adults with PPF.10 Patients receiving JASCAYD 18 mg or 9 mg showed an adjusted mean reduction of 86 mL and 69 mL in FVC, respectively, compared to 152 mL with placebo.10 The respective treatment difference compared with the placebo group was 65 mL (95% CI: 30, 101) and 83 mL (95% CI: 48, 118).
Over the blinded duration of the trial (up to 109 weeks), there was no statistically significant treatment difference in the hazard ratio (HR) for the JASCAYD 18 mg or 9 mg groups compared to placebo for the key secondary composite endpoint (JASCAYD 18 mg or 9 mg groups, respectively, compared to placebo: HR 0.77 (95% CI: 0.59, 1.01) and HR 0.88 (95% CI: 0.68, 1.14).10 An exploratory analysis over the blinded trial duration (up to 109 weeks) indicated a nominally significant reduction in the risk of acute ILD exacerbations with JASCAYD 18 mg versus placebo (HR 0.60 [95% CI: 0.38, 0.94]), and a numerical reduction in the risk of hospitalization for respiratory cause with JASCAYD 18 mg versus placebo (HR 0.82 [95% CI: 0.61, 1.11]).10
Additionally, in the FIBRONEER™-ILD trial population, the HRs for all-cause mortality assessed until the end of the trial (up to 114 weeks) for JASCAYD 18 mg and 9 mg compared to placebo were 0.51 [95% CI: 0.34, 0.78] and 0.51 [95% CI: 0.34, 0.78], respectively. These results were not prespecified for multiplicity control.10
The most common adverse reactions in patients with PPF treated with JASCAYD were generally consistent with those observed in IPF.10
Diarrhea was more common in patients using JASCAYD with concomitant nintedanib. In patients taking nintedanib, diarrhea occurred in 49%, 50%, and 37% of patients treated with JASCAYD 18 mg twice daily, JASCAYD 9 mg twice daily, and placebo, respectively. In patients without concomitant use of nintedanib, diarrhea occurred in 27%, 16%, and 16% of patients using JASCAYD 18 mg twice daily, JASCAYD 9 mg twice daily, and placebo, respectively. In FIBRONEER™-ILD, diarrhea was the most common adverse reaction associated with treatment discontinuation and occurred most frequently in patients treated with JASCAYD 18 mg (4%) or JASCAYD 9 mg (3%) with background antifibrotic therapy versus patients receiving placebo (1%) and background antifibrotic therapy.
Diarrhea leading to treatment discontinuation occurred in 1% of patients treated with JASCAYD 18 mg twice daily and in no patients treated with JASCAYD 9 mg or placebo without concomitant use of nintedanib. In most patients treated with JASCAYD, diarrhea was of mild to moderate intensity and generally occurred within the first three months of treatment.
Weight decrease was more common in patients who received JASCAYD concomitantly with nintedanib, which occurred in 12%, 10%, and 9% of patients treated with JASCAYD 18 mg twice daily, JASCAYD 9 mg twice daily, and placebo, respectively. In patients without concomitant use of nintedanib, weight decrease occurred in 13%, 8%, and 5% of patients treated with JASCAYD 18 mg twice daily, JASCAYD 9 mg twice daily, and placebo, respectively.
Among patients with PPF, neoplasms (benign, malignant, or unspecified) were reported in more patients with PPF treated with JASCAYD 18 mg (5%) or JASCAYD 9 mg (5%) than placebo (3%) over the entire study duration. Malignancies such as non-melanoma skin cancers and small cell lung cancer were observed in patients who received JASCAYD (basal cell carcinoma: JASCAYD 18 mg n=2 [1%] vs. JASCAYD 9 mg n=3 [1%] vs. placebo n=1 [0.3%]; squamous cell carcinoma of skin: JASCAYD 18 mg n=4 [1%] vs. JASCAYD 9 mg n=2 [0.5%] vs. placebo n=0; and small cell lung cancer: JASCAYD 18 mg n=4 [1%] vs. JASCAYD 9 mg and placebo n=0).
Less common adverse reactions in the PPF population following administration of JASCAYD include atrial fibrillation (3% JASCAYD 18 mg twice daily, 2% JASCAYD 9 mg twice daily, and <1% placebo).
What JASCAYD Means for the Community
“JASCAYD’s approval has been helpful in adding more tools to the limited kit available to treat patients,” shares Dr. Zaman. “The landscape for treating IPF and PPF really hadn’t changed much until the approval of JASCAYD for both IPF and PPF last year.”
“JASCAYD’s approval represents an important expansion of therapeutic options for patients with IPF or PPF,” adds Dr. Zapantis.
IMPORTANT SAFETY INFORMATION (CONTINUED)
DRUG INTERACTIONS
Effects of Other Drugs on JASCAYD
- Strong CYP3A Inhibitors: Reduce the dosage of JASCAYD to 9 mg twice daily when used concomitantly with strong CYP3A inhibitors. Nerandomilast is a CYP3A substrate. Concomitant use of JASCAYD with a strong CYP3A inhibitor increases exposure of nerandomilast, which may increase the risk of JASCAYD adverse reactions.
- Moderate or Strong CYP3A Inducers: Avoid use of JASCAYD with strong or moderate CYP3A inducers. Nerandomilast is a CYP3A substrate. Concomitant use of JASCAYD with moderate or strong CYP3A inducers is expected to decrease exposure of nerandomilast, which may decrease the efficacy of JASCAYD.
- Pirfenidone: Recommended dosage of JASCAYD is 18 mg twice daily when used concomitantly with pirfenidone. Do not reduce the dosage to 9 mg twice daily. Concomitant use of JASCAYD with pirfenidone decreases exposure of nerandomilast. When JASCAYD was used concomitantly with pirfenidone in patients with IPF in FIBRONEER-IPF, efficacy was not observed with the JASCAYD 9 mg twice daily dosage.
USE IN SPECIFIC POPULATIONS
- Pregnancy: Advise pregnant women and females of reproductive potential of the potential risk of fetal loss. Advise female patients to contact their healthcare provider if they become pregnant or suspect they may be pregnant during treatment with JASCAYD.
- Lactation: The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for JASCAYD and any potential adverse effects on the breastfed infant from JASCAYD or from the underlying maternal condition.
- Renal Impairment: Use of JASCAYD is not recommended in patients with end stage renal disease (eGFR <15 mL/minute/1.73 m2).
- Hepatic Impairment: Use of JASCAYD is not recommended in patients with severe (Child-Pugh Class C) hepatic impairment.
CL-JS-100019 4.17.2026
Please see full Prescribing Information for JASCAYD, including Patient Information.
References:
1 Sauleda J, Núñez B, Sala E, Soriano JB. Med Sci (Basel). 2018;6(4):110. DOI:10.3390/medsci6040110.
2 Kondoh Y, Inoue Y. Adv Ther. 2025;42(7):2988–3001. DOI: 10.1007/s12325-025-03215-6.
3 Raghu G, Remy-Jardin M, Richeldi L, et al. Am J Respir Crit Care Med. 2022;205(9). DOI: 10.1164/rccm.202202-0399ST.
4 Monthly Population Estimates for the United States: April 1, 2020 to December 1, 2022. U.S. Census Bureau, Population Division. Accessed May 8, 2025. Available at: https://www2.census.gov/programs-surveys/popest/tables/2020-2021/national/totals/NA-EST2021-POP.xlsx.
5 Jeganathan N, Sathananthan M. ERJ Open Res. 2021 Feb 7;8(1):00630-2021. DOI: 10.1183/23120541.00630-2021.
6 Fan Y, Bao H, Pimple P, Olson AL, et al. Ann Am Thorac Soc. 2026 Feb 1;23(2):208-218. doi: 10.1513/AnnalsATS.202503-262OC. PMID: 40986793.
7 Arcana R. et al. J Pers Med. 2023;13(11):1589.
8 FDA Press Release. October 2025. Accessed November 24, 2025. Available at: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-drug-treat-idiopathic-pulmonary-fibrosis.
9 FDA Press Release. December 2025. Accessed February 4, 2026. Available at: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-drug-treat-chronic-progressive-lung-disease.
10 JASCAYD® (nerandomilast). Prescribing Information. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc; 2026.
11 Drugs@FDA: FDA-approved drugs. US Food and Drug Administration. Accessed October 8, 2025. Available at: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&Ap plNo=205832.
12 Drugs@FDA: FDA-approved drugs. US Food and Drug Administration. Accessed August 13, 2025. Available at: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=022535.
13 Pulmonary Fibrosis Medications. American Lung Association. Accessed January 26, 2026. Available at: https://www.lung.org/lung-health-diseases/lung-disease-lookup/pulmonary-fibrosis/patients/how-is-pulmonary-fibrosis-treated/medications.
14 Mulhall A, Droege C, Ernst, N, et al. Expert Opinion on Investigational Drugs. 2015 Sep 20; 24(12), 1597–1611. DOI: https://doi.org/10.1517/13543784.2015.1094054.
MPR-US-104031 5/26
The MedPage Today Editorial team was not involved in the creation of this content.
Source link : https://www.medpagetoday.com/ad-insights/industry-clinic/121022
Author :
Publish date : 2026-05-19 16:00:00
Copyright for syndicated content belongs to the linked Source.






{kind=link}