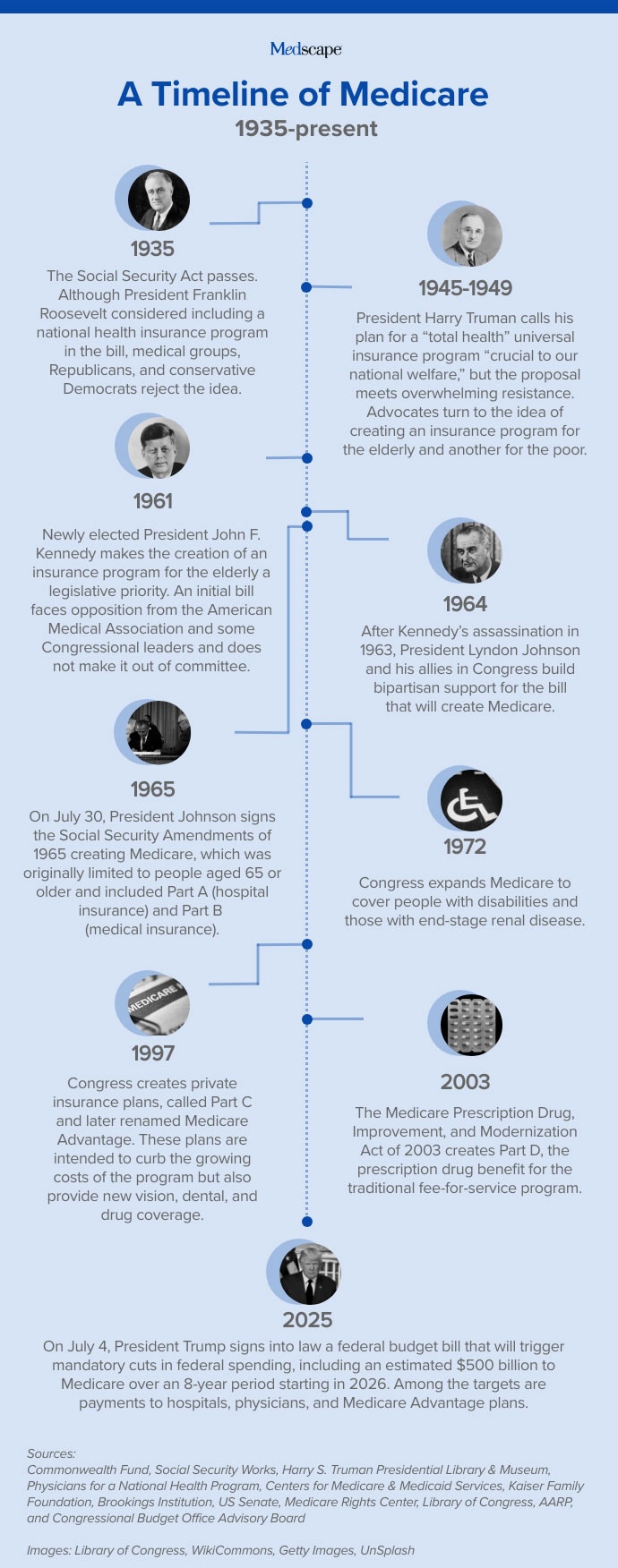
The creation of Medicare in 1965 was hailed as a watershed for the social safety net, offering millions of older Americans financial security and freedom from worry about their medical expenses. But critics of the legislation cast dire warnings about what the law would do to the nation’s physicians, the doctor-patient relationship, and even the country’s way of life.
Who was right? To mark the 60th anniversary of Medicare, Medscape Medical News asked leaders in healthcare, American history, and public policy to reflect on the words of the program’s earliest champions and critics. Comments have been edited for length and clarity.

Then-Senator John F. Kennedy, spoke in support of a national insurance program for the elderly at an event on August 14, 1960:
“Three out of every five of these [people over age 65] — more than 9.5 million people — must struggle to survive on an income of under $1000 a year. …This poverty and hardship turn into heartbreak and despair when illness threatens. Medicines and drugs are more expensive than ever before — hospital rates have more than doubled — doctor bills have skyrocketed. …Those over 65 suffer from chronic diseases at almost twice the rate of our younger population — they spend more than twice as many days restricted to bed — and they must visit a doctor twice as often.”
Commentary
Keith Wailoo, PhD, Henry Putnam University professor of history and public affairs at Princeton University and past president of the American Association for the History of Medicine:
“An important backdrop behind JFK’s comment is reflecting 10 years prior on the failure of President Harry Truman’s national health insurance proposals. The frustrations and the stories he’s telling were evident after World War II.

“He’s describing a landscape where — in the course of the war — private insurance became more attached to employment, wage freezes meant that companies couldn’t raise wages, unions lobbied and employers argued that benefits could be increased, and as a result of a momentous Supreme Court ruling, health insurance became increasingly a byproduct of employment. Healthcare costs were rising, and insurance was becoming a passage point to getting hospital care.
“The face of the poor and medical needy were the elderly by 1960. They were not working, and because of advancing life expectancy, there was more infirmity and yet they were locked out of the system.
“So we’ve recreated the world, and with that we have also changed people’s expectations about what they can hope for.”
In 1961, Ronald Reagan released a speech against a proposed bill that would cover hospital costs for the elderly. The effort was later revealed to be part of a campaign by the American Medical Association (AMA) to quash efforts to create a national health insurance program. Reagan said:
“[The bill] was simply an excuse to bring about what they wanted all the time, socialized medicine. … First, you decide that the doctor can have so many patients, they’re equally divided among the various doctors by the government. But then the doctors aren’t equally divided geographically. So a doctor decides he wants to practice in one town, and the government has to say to him, ‘You can’t live in that town. They already have enough doctors,’ and from here, it’s only a short step to dictating where he will go.”
Commentary
Reid B. Blackwelder, MD, associate dean for graduate medical and continuing education, DIO, Quillen College of Medicine, East Tennessee State University, and past president of the American Academy of Family Physicians:
“Reagan’s warning that nationalized health insurance would lead to government direction for where physicians practice has not happened. Physicians have the freedom to accept insurance or not and to practice anywhere they want. Sadly, our country is facing increasing healthcare deserts for various reasons.

“We already had a serious and growing access problem for patients. Now, patients in rural areas especially are losing even more access to primary care physicians and specialists as rural hospitals shut down and physicians like obstetricians stop practicing outside of urban areas.
“Ironically, Medicare is perhaps the most lenient health insurance in terms of providing that freedom of choice Reagan described for patients. Because Medicare is popular and widely accepted by patients and physicians, patients can readily choose the physician they want, including subspecialists. On the other hand, for-profit insurance has created significant limits on which physicians a patient may select based on acceptance of that insurance and cost. It can be difficult for a patient to see the physician of their choice.”

Edward Annis, MD, chairman of the AMA’s speakers’ bureau — and later president of the association — appeared in a televised May 21, 1962, address about the proposed King-Anderson bill, an early iteration of what would become the legislation that created Medicare. Annis said:
“It wastefully covers millions who do not need it, it heartlessly ignores millions who do need coverage. It is not true insurance. It will create an enormous and unpredictable burden on every working taxpayer. It offers sharply limited benefits. And it will serve as a forerunner of a different system of medicine for all Americans.”
Commentary
Jonathan Oberlander, PhD, professor of social medicine at the University of North Carolina at Chapel Hill, and editor of the Journal of Health Politics, Policy and Law:
“The AMA’s overheated rhetoric against Medicare did not age well. Doctors would later face challenges to their clinical autonomy, as Annis had feared, but that intrusion came from private managed care insurers trying to control skyrocketing costs, not Medicare.
“Yet the AMA was right about one thing. Although they didn’t admit it during the 1960s, Medicare’s architects saw the program as the first step to universal health insurance, and after covering the elderly, they hoped to next turn to children and eventually cover everyone via government insurance. Medicare for All was the aspiration.
“That did not happen, and although Medicare expanded eligibility in 1972 to cover persons with permanent disabilities and end-stage renal disease — six decades after the program’s enactment — its primary beneficiaries are still older Americans, an outcome that would have stunned its creators.
“After Medicare’s enactment in 1965, the AMA’s opposition to the program faded, much to Annis’ consternation. Forty years later, he still expressed regret that the association did not take a more ‘militant’ stand highlighting the program’s problems.”

Annis continued:
“This King-Anderson Bill is a cruel hoax and illusion. … It will come between the patient and his doctor.”
Commentary
Reid B. Blackwelder, MD, associate dean for graduate medical and continuing education, DIO, Quillen College of Medicine, East Tennessee State University, and past president of the American Academy of Family Physicians
“The special and powerful relationship between patients and physicians is a real thing. Medicare did not damage it. Other insurance coverage did not damage it. Having any insurance coverage is one of the foundations of getting to good health outcomes. The other is having a source of comprehensive care. Patients need both.
“The very real threat to the physician-patient relationship that is accelerating today is from legislative intrusions into the patient room. When laws are passed that make even just exploring options with patients around things like reproductive health a criminal offense, government has overstepped.
“When laws are enacted that require a physician to call their lawyer rather than a specialty consult before providing life-saving care, we have entered a new and dangerous era of governmental oversight. Recent laws have done more damage to the sanctity of the physician-patient relationship that Medicare actually helped improve.”

Representative Durward Gorham Hall, MD (R, Missouri), made these remarks below during debates on Medicare in the House of Representatives:
“This conflict is testing whether art and science of medicine will be permitted to grow and flourish in freedom and competitively, or whether progress in medicine will be stunted and shriveled by an excess of Government control.”
Commentary
Jonathan B. Jaffery, MD, MS, MMM, chief healthcare officer at the Association of American Medical Colleges:
“By supporting the training of physicians, Medicare helps create the physician workforce for future generations of Americans, crucial for the care of an aging population. And through iterative developments over the last 60 years, such as Coverage with Evidence Development or the Center for Medicare and Medicaid Innovations, the Medicare program — coupled with federal investments in biomedical research — has been able to support innovations in both medical technologies and models of care delivery that continue to improve the lives and well-beings of millions.

“The reality is, prior to 1965, many elderly Americans with healthcare needs were forced to rely on financial support from their families or spend all their life’s savings, hope for charity care, or forgo care altogether. And of course, the cost of care has only skyrocketed, so that in 2025 even very high-net worth individuals would struggle to cover the costs of a lengthy hospitalization or extended illness, let alone the price tag of many new life-saving medications.”
Hall continued:
“The result will inescapably be third-party intrusion in the practice of hospitalization and medicine. His diagnostic and therapeutic decisions would be subject to disapproval by those controlling the expenditure of tax money.”
Commentary
G. William Hoagland, senior vice president, Bipartisan Policy Center, former executive at Cigna, and former US Senate staffer
“Representative Hall was prescient in his observation about the future of healthcare resulting from the creation of Medicare. The 60-year history of the Medicare program, particularly since the enactment of the Tax Equity and Fiscal Responsibility Act in 1982, the Medicare Modernization Act in 2003, and the Patient Protection and Affordable Care Act in 2010, has resulted in the ‘corporatization’ of healthcare.

“Today, Medicare Advantage, dominated by ‘third-party’ corporate insurance companies, has transferred the physician’s independent decisions to actuaries and corporate financial decision makers. The result has also been horizontal consolidation of what were locally controlled entities to nationally or regionally controlled corporations along with vertical consolidation of payers and care delivery entities.
“The impact of these changes, along with dramatic scientific advances in diagnosis with advanced treatment protocols, precipitating higher healthcare utilization, has not been to reduce costs but to in fact increase healthcare costs.”

Following passage of the Social Security Amendments of 1965 out of the Senate by a vote of 68-21, President Lyndon B. Johnson said:
“It will help pay for care in hospitals. If hospitalization is unnecessary, it will help pay for care in nursing homes or in the home. And wherever illness is treated — in home or hospital — it will also help meet the fees of doctors and the costs of drugs.”
Commentary
Bruce Leff, MD, professor of medicine and director of the Center for Transformative Geriatric Research, Johns Hopkins University School of Medicine in Baltimore:
“Johnson’s statement regarding care at home was appropriate for the mid-1960s. To this day, skilled home healthcare remains the most used home-based service by Medicare beneficiaries.
“Since Medicare was enacted, a bevy of evidence-based home care delivery models have been developed and proven. These home-based models span the care continuum including home and community-based services, home-based primary care, transitional care, and home-based palliative care.

“Unfortunately, Medicare payment policies incentivized the centralization of care in facilities and a facility-centric culture of care delivery. Care delivery hasn’t kept pace with the needs of an aging population with a high prevalence of homebound older Americans or with the advances that enable even hospital care to be delivered to patients in their preferred setting, their homes.
“The hospital of the future will comprise of emergency departments, operating rooms, and intensive care units. Most other care can and will be provided in the home setting. We have all the pieces to develop this future home-based care vision. Achieving this vision will require a culture shift with associated payment and regulatory enhancements, ongoing attention to improvements in technology, logistics, and data management.”
Johnson continued:
“Older citizens will no longer have to fear that illness will wipe out their savings, eat up their income, and destroy lifelong hope of dignity and independence. For every family with older members, it will mean relief from the often-crushing responsibilities of care.”
Commentary
Gretchen Jacobson, PhD, vice president, Medicare program, Commonwealth Fund:

“One third of Medicare beneficiaries said in 2023 that it was difficult to afford healthcare costs. More than 1 in 5 beneficiaries reported in 2023 delaying or skipping needed healthcare because of the cost. Similarly, some Medicare beneficiaries trade off paying for other necessities to pay for needed healthcare. The lack of a limit on out-of-pocket spending on hospital and physician services for traditional Medicare has, for most traditional Medicare enrollees, necessitated purchasing supplemental insurance coverage. Yet, the limited availability of this supplemental coverage has resulted in more beneficiaries enrolling in Medicare Advantage and high underinsurance rates among those in traditional Medicare without supplemental coverage.
“Medicare beneficiaries who do not have a family caregiver and cannot afford to pay out-of-pocket for a formal caregiver are typically forced to deplete their financial resources to qualify for Medicaid coverage, the largest payer for long-term care in the US.”
Hoagland reported owning shares in CIGNA. Leff reported receiving personal consulting fees from Chartis Healthcare, the Aligned Health Group, the Kenes Group, stock options via membership on clinical advisory boards to Dispatch Health, Patina Health, and Pager Health. Jaffery, Oberlander, Jacobson, Wailoo, and Blackwelder report no relevant financial disclosures.
Source link : https://www.medscape.com/viewarticle/johnson-reagan-experts-unpack-rhetoric-framed-medicares-2025a1000jwo?src=rss
Author :
Publish date : 2025-07-29 14:01:00
Copyright for syndicated content belongs to the linked Source.









{kind=link}