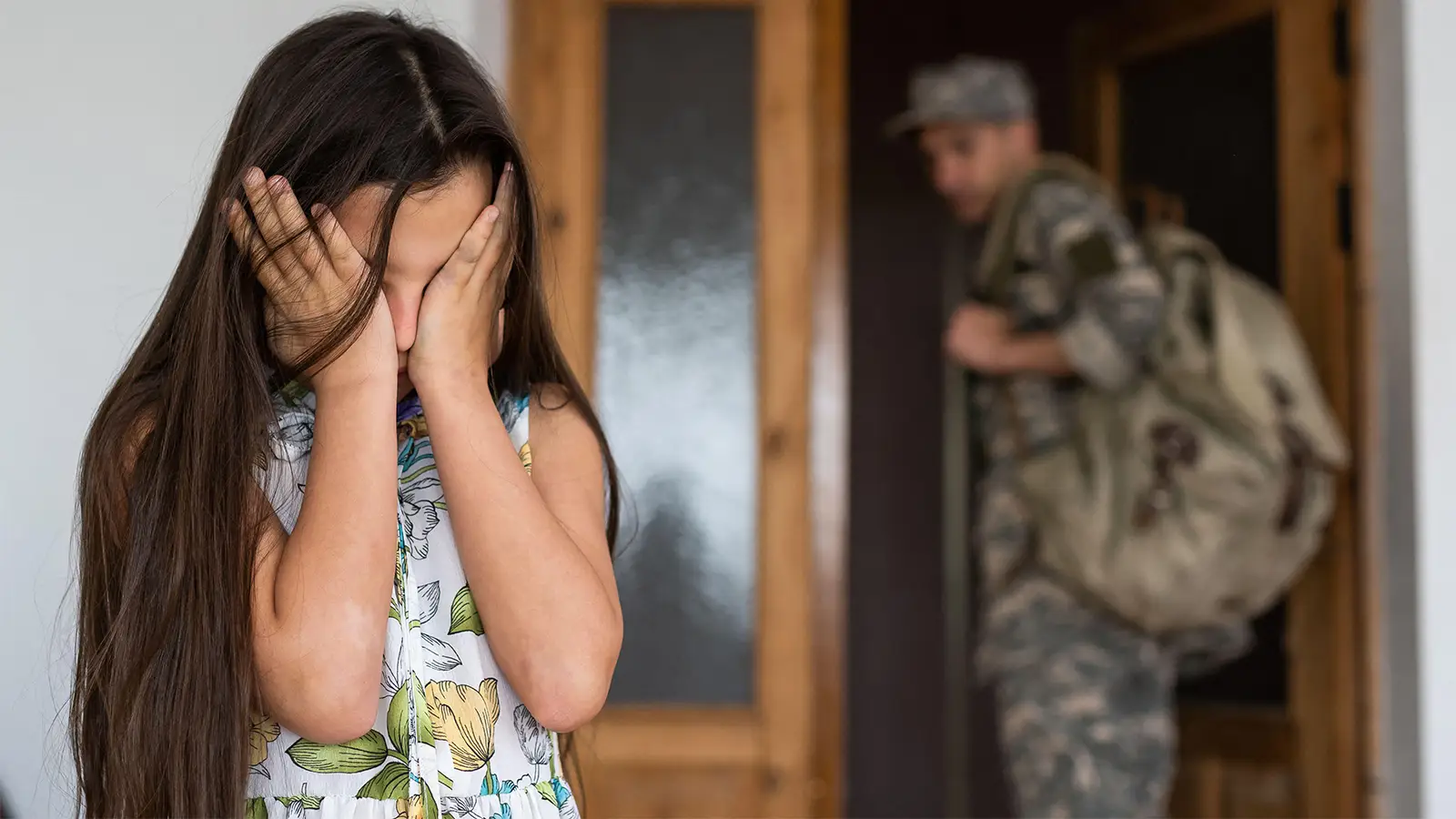
She was 7 years old. She had heard about the war in Iran from an older sibling, and by the next morning she had carried that knowledge, wordlessly, into my office. As her mother sat beside her, she asked the question that had been sitting in her chest all night.
“Mommy, are we going to die?” she said, her small brow furrowing beneath brown curls, distress taking over her face.
Her mother suppressed a sharp intake of breath, swallowed slowly, and replied: “No, sweetheart. This is happening far, far away.”
Then the mother looked at me. That look contained two things at once: the knowledge that war could not be guaranteed to stay far away, and something quieter and more universal, a recognition that children everywhere are just children. Whether in Iran or here.
That child is not unusual — she is a version of what is happening, right now, across this country. Distress that is going largely unnamed because the national conversation about the war the U.S. and Israel launched against Iran on February 28 — the culmination of more than a year of escalating regional conflict — has covered geopolitics, oil prices, military strategy, and body counts. It has not covered what this war is doing to children here, to American children.
There are five overlapping populations I keep thinking about. None of them has received the public attention they deserve.
The Children Whose Parents Are Deployed
This is the best-documented group. More than 2 million American children have had a parent serve in Iraq or Afghanistan. Now deployments are happening again. Children with a deployed parent show elevated rates of anxiety, depression, behavioral disorders, and acute stress reactions. The strongest predictor of how a child fares is the mental health of the parent who stays behind. When that caregiver is overwhelmed, the child absorbs it. The stress transmits. Return from combat is its own crisis, with reintegration straining families in ways that can escalate to maltreatment.
These families are navigating all this right now. Quietly.
The Iranian-American Children
There are approximately 750,000 Iranian Americans in the U.S. They are watching bombs fall on a country that is, for many, both a place they fled and a place they still love. Family message chains go silent for days. When something breaks through from behind Iran’s near-total internet blackout, it is a fragment: Where did they hit?
There is no direct research on Iranian-American children during this specific conflict. But the broader literature identifies family separation, disrupted communication, and inability to ensure loved ones’ safety as among the most harmful pathways to adverse outcomes in conflict-affected diaspora communities. This is a plausible mechanism, not established fact. For these children, the war lands on identity, family connection, and sense of safety simultaneously.
The Jewish-American Children
Jewish-American children face this war through a documented surge in antisemitism, vicarious trauma, and the possible activation of intergenerational wounds. Following the Hamas attack on Israel on October 7, 2023, one study that examined Jewish parents in California found that participants had significant increases in stress, anxiety, and depression, with perceived antisemitism partially explaining these changes. There is no published research on the mental health of Jewish-American children in the wake of those attacks, a gap that itself speaks to how overlooked this population has been. The American Academy of Pediatrics (AAP) recognizes that religious bigotry magnifies trauma risk. For many Jewish children, this war does not arrive in a vacuum — research suggests intergenerational transmission of trauma vulnerability in descendants of Holocaust survivors, though the precise mechanisms remain contested. It arrives into a family history.
The Palestinian-American Children
Palestinian-American children face a parallel burden — one that predates this war but is compounded by it. Many have already lost relatives in Gaza, live with severed family communication, and carry unprocessed grief, while facing a documented surge in anti-Palestinian and anti-Muslim hostility since October 2023.
The current conflict with Iran has intensified regional instability and extended the climate of fear. Research on diaspora populations demonstrates that conflict in one’s country of origin or heritage region profoundly impacts mental well-being even from abroad, yet there is no published research specifically on Palestinian-American children. Like Jewish-American children, they are present in our schools and our clinical offices, and they too have been invisible in this conversation.
Every Other American Child
This is the largest group and the least studied. The evidence on ambient war exposure is genuinely limited — most studies are cross-sectional and involve children with some cultural proximity to the conflicts they watch. With those caveats stated: media exposure to war produces measurable distress and posttraumatic symptoms in children with no direct exposure, and adolescents who watch armed conflict on social media show psychological distress that optimism and self-mastery (the ability to control one’s thoughts, emotions, and behaviors) do not appear to moderate.
On February 28, the morning the Iran war began, the Shajareh Tayyebeh girls’ elementary school in Minab, Iran, was struck. The attack killed at least 168 children and 14 teachers. Multiple investigations have pointed to U.S. responsibility, though the findings remain contested. Most of the dead were girls between 7 and 12 years old — the same age as my patient with the brown curls.
Those images are on TikTok. An American teenager who picked up their phone that morning encountered graphic war footage before breakfast. And unlike a parent who can contextualize, adolescents are doing much of this processing alone, without the neurological equipment to regulate what they are absorbing.
The AAP guidelines are careful to distinguish between distress — which is common and expected — and clinical disorder, which most children will not develop. The goal is not to pathologize normal reactions to abnormal events, but to recognize them, name them, and ensure children have adults to help them metabolize what they are carrying.
What This Asks of Us
This war arrived into a domestic landscape already structurally compromised for children — with the Substance Abuse and Mental Health Services Administration (SAMHSA), school-based programs, and community behavioral health funding under active dismantlement — while economic stress compounds the burden on families through well-established transmission pathways.
If you are a clinician: screen for this. Ask what children are seeing online, what they’re hearing at home, whether they have relatives in Iran or Israel, whether a parent is deployed. Ask about antisemitism. Ask about the feeling of not being seen. For children with identified trauma exposure, the UCLA PTSD Reaction Index Brief Form and the Child Trauma Screening Questionnaire are available for triage. Children frequently protect their parents from knowing how frightened they are — the clinical encounter matters. For the subset who develop clinical disorders, trauma-focused cognitive behavioral therapy has the strongest evidence base; early intervention can prevent chronic PTSD.
If you are a parent: open the conversation. Not to alarm, but to accompany. Children who are allowed to ask questions, to name their fear, and to be met with honesty rather than managed with reassurance tolerate uncertainty better. Psychological first aid approaches — listening, maintaining routines, reinforcing safety — are within reach of every caregiver. Presence is protective.
If you are a policymaker: most children are resilient and will not develop chronic psychopathology. But a significant subset likely will, and the research from every previous conflict is unambiguous: the effects last for years. The time to fund child and adolescent mental health infrastructure is before the crisis, not the week after it’s been dismantled.
The girls of Minab were not abstractions. Iran held a mass funeral for them in a public square; their photographs were published in a collage. Our children are watching us figure out what to do with that. They are doing it in real time, on platforms designed for engagement rather than emotional safety, without nearly enough adult presence, and in an institutional context ill equipped to receive them.
The 7-year-old in my office asked her mother if they were going to die. Her mother told her this was happening far, far away.
It is. And it isn’t. Every war finds its way home — in the nightmares of deployed parents’ children, in the silence of Iranian-American families waiting for a message that may not come, in the Jewish child who walks into school braced for something she can’t yet name, in the phone screens of teenagers absorbing images they have no framework to hold.
We should say so.
Jonathan Slater, MD, is a clinical professor of psychiatry at Columbia University Irving Medical Center.
Source link : https://www.medpagetoday.com/opinion/second-opinions/120556
Author :
Publish date : 2026-03-30 17:54:00
Copyright for syndicated content belongs to the linked Source.










{kind=link}