A man in his early 60s became so progressively weak over 7 years that he could no longer walk — and didn’t realize he had fractured both femoral necks and 11 ribs.
The cause: a tumor hiding in his leg.
Clinicians had attributed his worsening muscle weakness and diffuse pain to small-fiber neuropathy and chronic Lyme disease, but treatments including intravenous immunoglobulin and antibiotics produced no improvement. By the time he presented to a hospital with new right-sided pleuritic chest pain, he had been largely bedridden for 9 months.
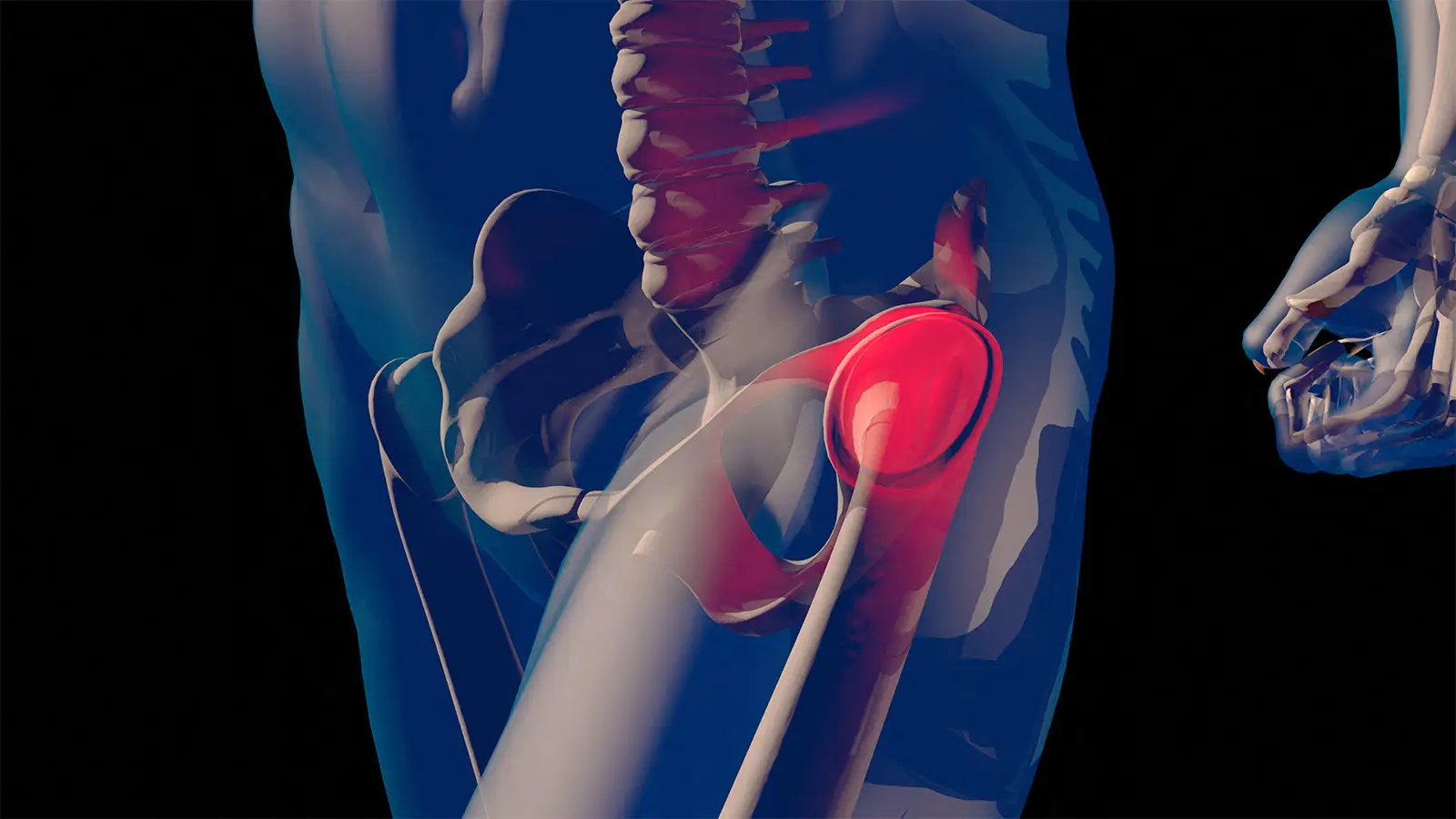
The underlying diagnosis, as detailed by Laura R. Glick, MD, of Harvard Medical School and Massachusetts General Hospital in Boston, and colleagues in BMJ Case Reports, was tumor-induced osteomalacia (TIO) caused by a 15 x 9 mm phosphaturic mesenchymal tumor (PMT) lodged in his left femoral neck — a small, slow-growing lesion that had been silently dismantling his skeleton for years.
PMTs are rare, usually benign tumors that secrete fibroblast growth factor 23 (FGF23), a key regulator of phosphate homeostasis. Excess FGF23 causes renal phosphate wasting, low levels of active vitamin D, and impaired bone mineralization, resulting in osteomalacia and fragility fractures. Because symptoms are nonspecific and serum phosphate is not routinely measured, diagnosis is often delayed — sometimes for years. PMTs have been initially misdiagnosed in up to 95% of cases.
In this case, the COVID-19 pandemic was a contributing factor, said Glick, who treated the man early during his hospitalization. Because he relied heavily on telehealth visits with clinicians over 3 years, “nobody was able to appreciate how progressive his weakness had become,” Glick told MedPage Today.
Imaging on admission revealed chronic bilateral femoral neck fractures, a left proximal femoral diaphyseal fracture, and 11 posterior right rib fractures. Laboratory testing showed severe hypophosphatemia at 0.5 mmol/L, elevated alkaline phosphatase, low 1,25-dihydroxyvitamin D, and elevated intact FGF23 levels. Calculations of fractional excretion of phosphate and tubular maximum reabsorption of phosphate confirmed inappropriate renal phosphate wasting.
“The combination of acquired (vs congenital) weakness and bony pain (with or without fracture) is classic for a phosphate wasting disorder,” co-author Sherri-Ann Burnett-Bowie, MD, MPH, also of Harvard Medical School and Massachusetts General Hospital, told MedPage Today. “Once the new diagnosis of hypophosphatemia was made, the associated low 1,25-dihydroxyvitamin D level was classic for tumor-induced osteomalacia.”
Functional imaging with copper-64 DOTATATE PET/CT identified increased uptake in the left femoral neck and at the gastroesophageal junction, two potential culprits that needed to be sorted out. To distinguish between the two sites, physicians performed selective venous sampling. FGF23 concentrations were markedly elevated in the left lateral femoral circumflex vein compared with other sampled sites, localizing the source to the femur. Endoscopy later showed the gastroesophageal uptake was due to a hiatal hernia — not the tumor.
The patient underwent resection of the femoral lesion with total left hip arthroplasty. Histopathology confirmed a PMT.
The recovery was striking. Within a week of surgery, his serum phosphate and FGF23 levels normalized. After a month, he was able to stand and walk with two canes for the first time in nearly a year. Six months after surgery, he could go to the grocery store for the first time in 5 years. At 1-year follow-up, he was walking around the block with one cane — with his grandchild — and reported a significant reduction in pain.
The case underscores the diagnostic challenge of TIO. Recurrent fractures, bone pain, and muscle weakness are common presenting features, yet serum phosphate — a key clue — is frequently overlooked. One large retrospective series found that 96% of TIO patients presented with recurrent fractures, 79% with body aches and pain, and 50% with weakness — yet the diagnosis was still routinely missed, the authors noted.
Localization can also be difficult, as these tumors are often small and may arise in bone or soft tissue, most commonly in the lower extremities or head and neck. Somatostatin receptor-based imaging such as gallium-68 or copper-64 DOTATATE PET is currently recommended, followed by high-resolution MRI or CT and venous sampling when needed.
Complete surgical resection typically results in rapid biochemical correction. For unresectable or nonlocalizable tumors, however, options include oral phosphate and calcitriol supplementation, or burosumab (Crysvita), a monoclonal antibody targeting FGF23, which was approved by the FDA in 2020.
Persistent hypophosphatemia in adults with fractures, bone pain, or unexplained weakness should prompt evaluation for renal phosphate wasting and consideration of this condition, the authors noted.
“The most important message is to listen to your patients, even if every lab is stone-cold normal,” Glick said. “Patients know themselves the best. If they come to you with progressive weakness or feeling ‘off,’ then chances are, they warrant additional work-up and testing.”
Source link : https://www.medpagetoday.com/casestudies/orthopedics/120112
Author :
Publish date : 2026-03-02 17:33:00
Copyright for syndicated content belongs to the linked Source.










{kind=link}